Pain, bleeding, fever - what symptoms actually mean something when it comes to ovarian torsion?
Well, in this retrospective case-control study looking at 221 patients from 2011 to 2022, Aiob et. al looked at a ton of history, physical exam, and ultrasound findings to see which ones correlated most strongly with ovarian torsion. They found that vomiting and reports of localized pain (v diffuse pain) were highly associated with surgery-confirmed ovarian torsion. In multivariate analysis, localized pain had an odds ratio of 4.36 and vomiting had an odds ratio of 2.38.
Additionally, on ultrasound findings, ovarian edema was much more likely to be present in torsion cases, with an odds ratio of 5.29.
This is a retrospective single center study that comes with all the limitations that these studies always come with, but let this be a reminder of what should trigger your Spidey-senses!
Additional note: We all know that torsion is a diagnosis that can only be confirmed by surgery, no matter what Doppler flow looks like, and this study just adds onto that pile of evidence: Doppler flow was not significantly different between patients who ended up having torsion and those who didn't. >60% of patients who ended up having torsion had normal flow, so like always, remember that a normal Doppler does not exclude torsion in a patient who you're worried about! Talk to OBGYN!
This paper outlines the long term effects of surviving a gunshot wound. The authors conclude:
“Firearm injury survivors frequently experience chronic pain, nerve injury, retained bullet fragments that may cause lead toxicity, physical limitations, and PTSD and are at risk for reinjury. In addition to supportive medical and psychiatric care, survivors of firearm injury may benefit from health care–based violence intervention programs.”
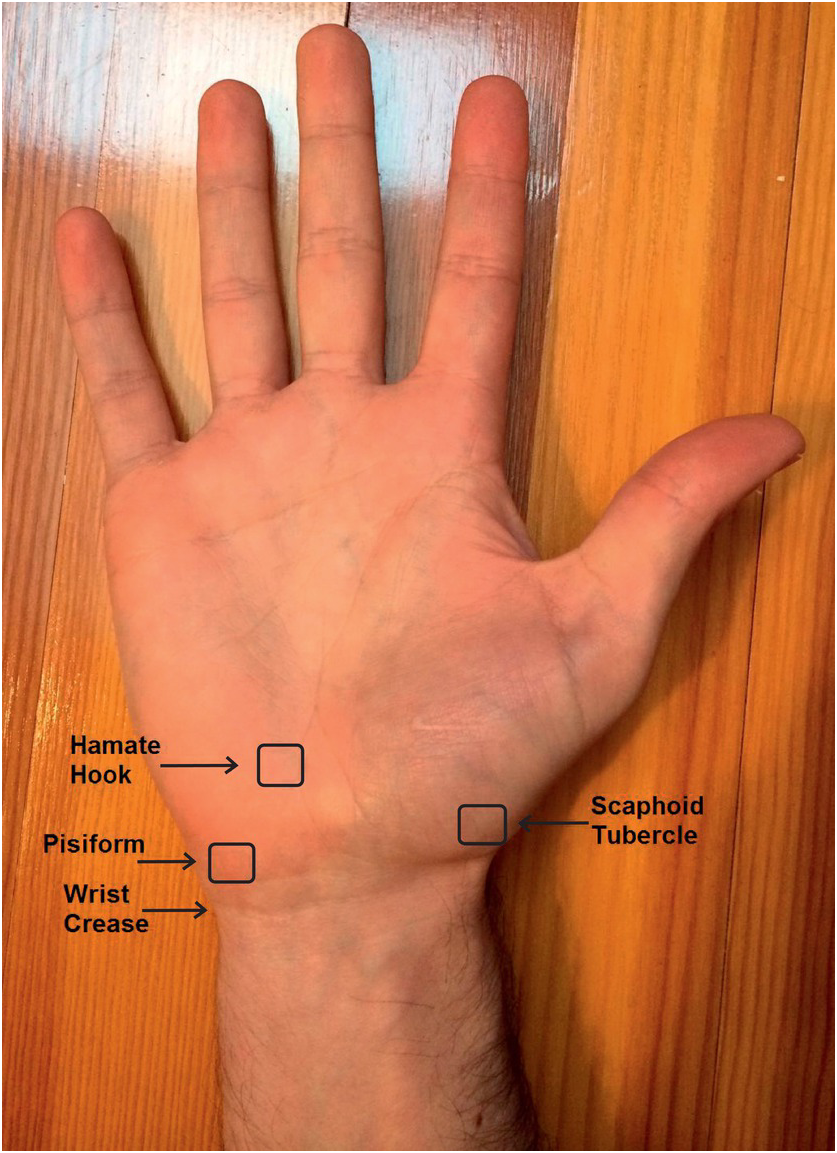
Scaphoid fractures
Make up almost 2/3rds of all carpal fractures
Fractures tend to be localized to 3 anatomic locations
Waist fractures make up 2/3rds. This may be diagnosed with anatomic snuffbox tenderness
Proximal pole fractures make up approximately 25%. This may be diagnosed with bone tenderness about a fingerbreadth distal to Lister’s tubercle
Distal fractures make up the remaining 10%. This may be diagnosed with tenderness at the volar prominence of the distal wrist crease
Imaging:
In addition to standard views of the wrist (PA/lateral/oblique) consider adding a scaphoid view. This imaging view is a PA film taken with the wrist in full pronation and ulnar deviation. This allows full visualization of scaphoid in its longitudinal axis. Also, this allows visualization of the area in question without the annoying overlap of adjacent carpal shadows
Have you ever wondered what happened to your mechanically ventilated patients who developed diarrhea. Apparently, a multicenter study involving 2650 patients from 44 ICUs in the US, Canada and Saudi Arabia investigated the prevalence of diarrhea among these patients.
This study was the Editor’s choice for June 2025.
Results:
The mean age for the population was 59.8 (16.5) years, with APACHE II Score of 22.0 (7.8). Up to 61% of the patients received vasopressors or inotropes on day 1, which mean these patients are relatively ill.
Up to 60% of patients had diarrhea during their ICU stay, with 15% had diarrhea on day 1 or 2.
Initiating laxatives and antibiotics (who in the ICU would not receive vitamin V and Vitamin Z?) were associated with increased risk of diarrhea: HR for laxatives 1.28 (1.13–1.44), p<0.001; HR for antibiotics 1.41 (1.20–1.67), P< 0.001.
Furthermore, enteral feeding with high/moderate protein concentration was also associated with diarrhea (HR 1.13, 1.00-1.28, P=0.045.
Not surprisingly, diarrhea was associated with higher number of C. Diff testing.
Although patients with diarrhea were associated with longer ICU stay (15 [10-23] days) vs. those without diarrhea (8 [6-12] days), it was not associated with higher mortality (HR 0.70, 95% CI 0.57-0.86, P<0.001)
Discussion:
1. The authors did not report the rates of positive C. Diff. infection in these patients during ICU stay, although they did report that for another study in this population, the rate of positive C. Diff. infection during ICU stay was 2.2%. If only 2.2% had C. Diff. infection while up to 60% had diarrhea. Consequently, for every 30 patients with diarrhea, only one patient had C. Diff. infection. Therefore, do we have to check C. Diff. in those ICU patients with diarrhea every time?
2. The authors hypothesized that patients with diarrhea had longer ICU stay and lower mortality because they survived long enough to develop diarrhea. Thus, diarrhea is bad for clinicians, but may not be too bad for patients?
Conclusion:
Diarrhea is common among invasively ventilated patients. Patients who received laxatives, antibiotics, enteral feeding with high protein amount are at higher risk for diarrhea.
Looking at a trauma database of over 3 million patients, 1% presented with prehospital hypothermia (<35 degrees C). These patients had longer hospital stays, higher resource utilization and higher mortality. Even isolated head injury patients with hypothermia had worse outcomes. Rewarming did increase survival slightly for all patients.
Take away: rewarm hypothermic trauma patients as soon as possible to improve mortality.
A scoping review of the literature regarding anxiety in older patients found the follow areas had the biggest impact on anxiety level:
“The variables most strongly associated with anxiety—either as risk or protective factors—are age, female gender, physical activity, physical health conditions, depression, perceived and family support, and social participation. New variables linked to anxiety include body mass index (BMI) and dietary habits.”
Asking questions related to these areas can give you a better picture of your patient’s risk for anxiety.
Looking at 140 patients retrospectively who had abdominal gunshot wounds with associated fractures, prophylactic antibiotics longer than three days did not offer any benefit in preventing fracture infection. Only two patients experienced fracture related infections and 65 total experienced any infection related complications.
From and ED standpoint, it appears reasonable to give a dose of antibiotics in this very rare subset of gunshot wound patients.
This prospective cohort study from Germany found an under triage rate of 58% of trauma patients over 70 years presenting to 12 trauma centers. One area that consistently lead to undertriage was not using a systolic blood pressure under 110 as a criteria for trauma team activation.
The older cohort had 3 times the mortality than younger, were more likely not to arrive by helicopter and mechanism was more commonly ground level fall. This study echos many others in USA and Australia. Better trauma triage criteria are needed for older patients.
PEEP is often titrated up along with FiO2 to increase oxygen saturation. Although the potential negative hemodynamic effect of high PEEP is often recognized, it is important to also note that high PEEP can also paradoxically worsen oxygen saturation.
The primary physiologic explanation for this phenomenon in a patient with pulmonary disease is due to the varying impact of PEEP on the intra- vs. extra-alveolar blood vessels. PEEP preferentially distends more normal/compliant lung which causes compression of intra-alveolar vessel at excessively high levels of PEEP. This causes pulmonary blood to be diverted to areas of lower vascular resistance (e.g. consolidated lung which is less distended due to its worsened compliance) and lower VQ matching. Essentially, blood flow to normal/healthy lung is decreased and is instead increased to diseased lung, worsening hypoxemia.
Bottom line:
High PEEP can potentially worsen hypoxemia and should be considered as an etiology for worsening oxygen saturation, particularly when the hypoxemia is out of proportion to the patient’s radiographic findings.
A retrospective, single Australian center review of 300 patients who had blunt cerebral vascular injuries found:
-9.8% had an inpatient CVA
-Most occurred in first 72 hours
-Those receiving no anti coagulation or antiplatelets had 28% CVA incidence.
-Those treated had a 3.6% CVA incidence (anti platelets were better than anti coagulation)
-Carotid artery injury was less common than vertebral artery but had higher frequency of CVA
-associated factors: low GCS, rib fractures, severe trauma
Take away: non-treatment of blunt cerebral vascular injuries had higher inpatient stroke risk. Antiplatelet agents such as aspirin and Clopidogrel performed better than anticoagulants
This paper looked at the literature regarding missed injuries in trauma patients. Missed injuries was defined as an injury discovered after the patient was discharged. Most of the missed injuries and causes are not novel but are worthy of remembering.
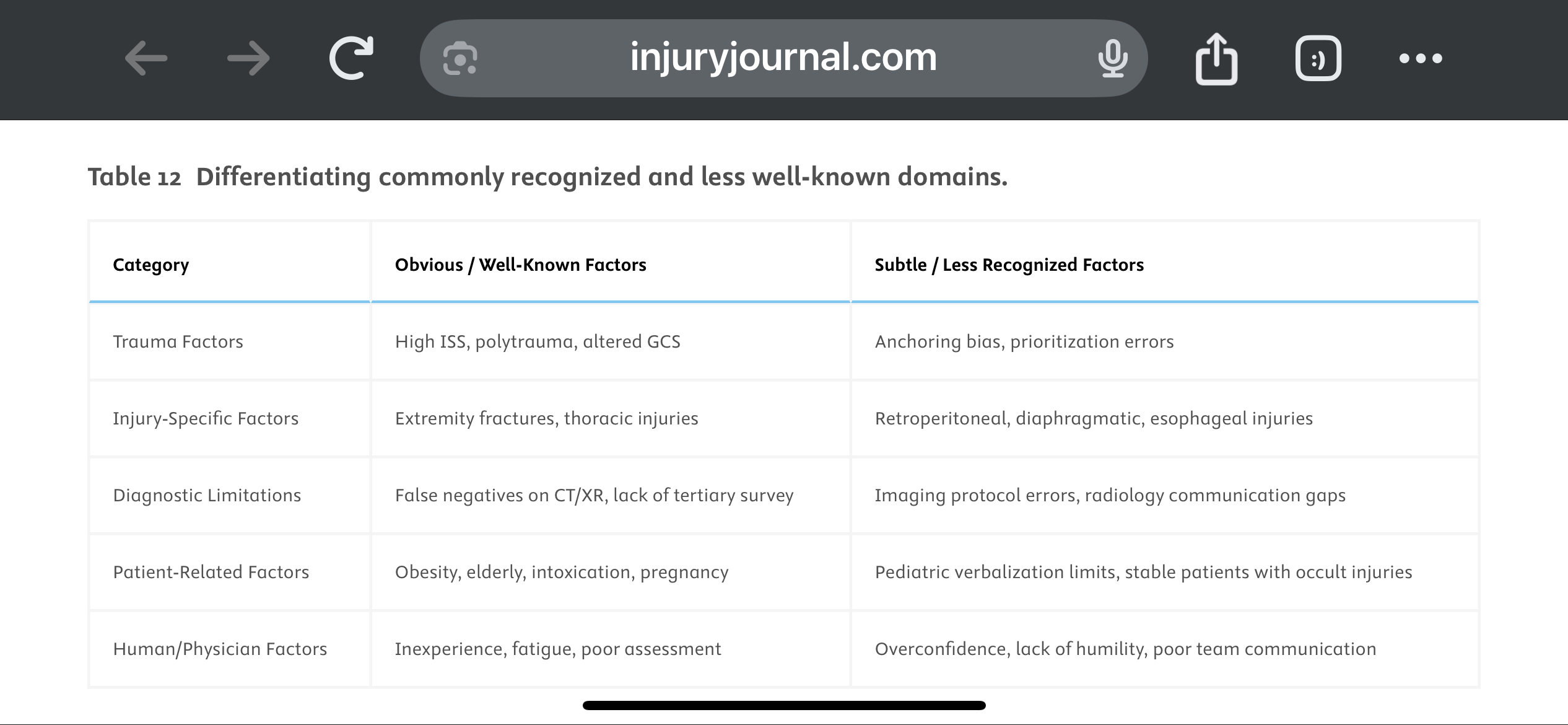
They suggest a Trauma Tertiary Survey helps prevent missed injury. “Tertiary Survey (TTS), which includes a thorough in-hospital re-examination and a review of diagnostic investigations within the first 24 h, has been shown to significantly reduce the occurrence of missed injuries (1–9 %) in severe trauma patients found after a primary and secondary survey.” This concept is similar to a discharge time out in emergency medicine where all data is reviewed, viral signals are confirmed normal and a team discharge is performed.
The paper offers these suggestions to avoid missed injuries:
1.
Standardize Tertiary Trauma Surveys (TTS).
2.
Be Cognizant of Cognitive Biases (e.g., Anchoring Bias).
3.
Repeat Imaging When Clinically Indicated.
4.
Use Protocolized Imaging Techniques (CT/MRI).
5.
Ensure Radiology-Trauma Communication.
6.
Prioritize High-Risk Populations.
7.
Implement Peer Review or Double-Check Systems.
8.
Encourage a Culture of Collaboration and Humility.
9.
Limit Provider Fatigue and Overload.
10.
Create Tailored Checklists for Subtle Injuries.
A recent study investigated the impact of pain management education counseling on postoperative opioid consumption.
Patients were randomly assigned to receive opioid limiting perioperative pain management education and counseling (intervention group) with instructions to take opioids “only as a last resort if the pain became unbearable.”
The control group received instructions to take opioids as needed for “severe pain” to” stay ahead of the pain.”
The primary outcome was the total morphine equivalents (TME) consumed in the 3 months after surgery.
Secondary outcomes included pain measured with the Numeric Rating Scale, sleep quality, opioid prescription refills, and patient satisfaction.
121 patients with a mean age of 29 years.
Both groups were told about potential adverse effects of opioids and were advised of alternative methods to control pain such as over-the-counter acetaminophen and ibuprofen.
60 patients in the treatment group consumed a mean of 46 mg TME versus 63.6 mg TME in the control group ( p < 0.001). There was no difference in the average score on the numeric rating scale in the first 14 days between groups. There was no significant difference in refill prescriptions between the groups. Sleep quality and patient satisfaction was also similar between groups.
Over 1/3 of patients in the intervention group took no opioids at all after surgery. In contrast, 9 out of 10 patients in the control group used all prescribed opioids after surgery.
Conclusion: Opioid limiting pain management education and counseling reduces opioid consumption without a change in reported pain. There may be a role for pain management education and counseling in emergency department patients in whom opiates are prescribed…similar to this study in perioperative orthopedic patients.
Secondary analysis of a multicenter, prospective, observational study ICE-CRASH study in Japan including adult patients admitted with moderate-to-severe accidental hypothermia between 2019 and 2022.
Some structural generalizability (median age 81 years!) issues with this study but well done overall.
Authors undertook some rather complex modeling to predict outcomes related to rapid rewarming, showing that “the rewarming rate and predicted probability of each outcome increased significantly up to 3°C/hr, but when the rewarming rate exceeded 3°C/hr, the predicted probability of each outcome was almost constant.”
Suggests that for those with severe hypothermia that an initially rapid rate of up to 3C/hr is a good target for a ceiling, but above this may be associated with less favorable risk:benefit ratio. Benefit in moderate hypothermia was not as clear.
Conclusion: The mode of rewarming in severe hypothermia should still be based on local protocols and capabilities (e.g. external, intravascular, extracorporeal rewarming) but the rate of rewarming up to 3C/hr is associated with better outcomes.
Shout out to UMEM alum Diane Kuhn, MD, PhD as the first author of this recent publication…
She and her colleagues examined the factors that contribute to ED patient experience scores, uncovering several which are not considered in the current CMS evaluative framework. See the editor's (our very own Stephen Schenkel, MD, MPP) capsule summary below:
What is already known on this topic? Medicare plans nationally standardized Emergency Department (ED) Patient Experience scores (ED
CAHPS) to allow comparison across sites.
What question this study addressed. Are there clinical and operational ED characteristics for which ED patient experience scores ought to be adjusted?
What this study adds to our knowledge. Based on 58,622 ED visits from one system, patients arriving in pain were less satisfied and those receiving radiologic studies had a positive experience.
How this is relevant to clinical practice. Influences on patient satisfaction are multifactorial and many are outside the control of the ED. Comparing EDs based on patient experience is complex and prone to misinterpretation.
As the authors point out, If patients placed in a hallway bed have a more negative experience simply due to the location in the department, or patients arriving in pain have a more negative experience regardless of ED care, then some EDs will face more challenges than others in achieving optimal patient experiences.
The current CMS evaluative framework may inherently disadvantage certain EDs, including those with limited physical space relative to their patient volumes, such as safety-net hospitals, or those that care for a high proportion of patients experiencing chronic pain. Is this fair? Does it reflect what CMS is trying to evaluate? Are there alternatives?
Kudos to Dr. Kuhn on her insightful publication and Dr. Schenkel for his expert editing!
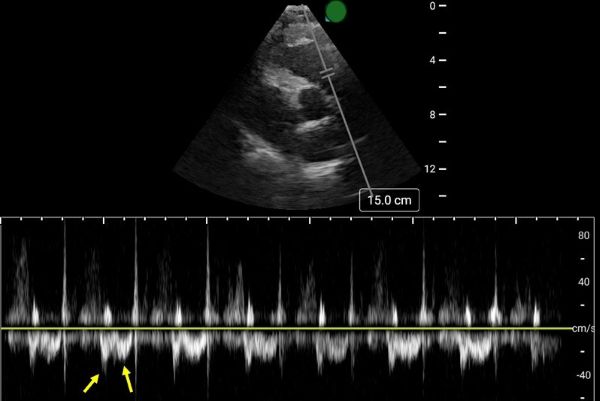
Early Systolic Notching and Pulmonary Embolism
A prospective multicenter study conducted across four academic emergency departments in Turkey evaluated the diagnostic accuracy of early systolic notching (ESN) in emergency department patients. Among the 183 patients included, 52.5% were diagnosed with pulmonary embolism (PE), while 19.7% exhibited the ESN finding. ESN demonstrated a sensitivity of 34% (95% CI: 25–45%) and a specificity of 97% (95% CI: 90–99%) for PE. Sensitivity increased to 69% in patients classified as high or intermediate-high risk. Overall, ESN exhibits moderate to high specificity but low sensitivity, consistent with other sonographic signs of PE. Notably, ESN may also be present in patients with chronic thromboembolic disease secondary to prior pulmonary hypertension.
How to Obtain ESN
To detect ESN, acquire a parasternal short axis view at the base of the heart to visualize the right ventricular outflow tract and pulmonic valve. Position the pulse wave Doppler gate just proximal to the pulmonic valve, with the cursor traversing the outflow tract. ESN is characterized by a sharp systolic spike with a notch, followed by a dome-shaped waveform
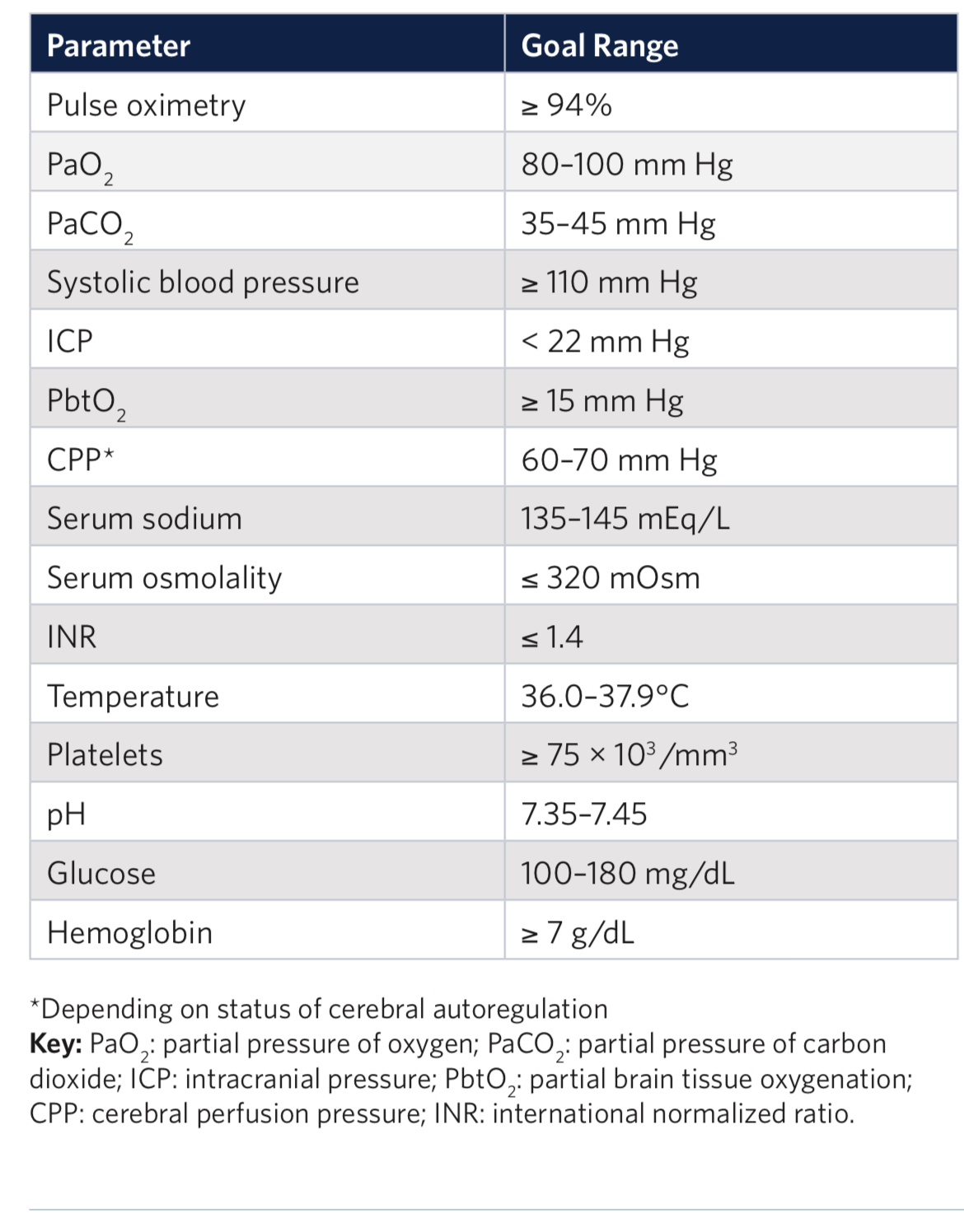
Outcomes in traumatic brain injury are improved when physiologic homeostasis is achieved as soon as possible after injury. Here are the American College of Surgeons’ recommendations. Note SBP over 110 and a hemoglobin over 7. A study looking at a more liberal transfusion target showed worse ARDS and no mortality benefit.
Trauma is a leading cause of death in pediatric patients. The Pediatric Traumatic Hemorrhagic Shock Consensus Conference Recommendations have stated that blood products are better than crystalloid and recommend the use of low titer type O whole blood (LTOWB) over individual components for pediatric traumatic resuscitation.
This study used the Trauma Quality Improvement Program Database to look at 1122 pediatric patients (< 18 years) over a 3 year period to retrospectively examine the impact of the ratio of whole blood and blood products given during the resuscitation of these patients. When at least 30% of the blood products delivered within the first 4 hours of resuscitation were low titer O whole blood, survival improved at the 6, 12 and 24 hour time mark.
The authors concluded that the observed survival benefit supports the greater availability and use of LTOWB during pediatric trauma resuscitation.
This was a multicenter retrospective cohort study over 6 years at 7 level one and two trauma centers.
1631 patients who had out of hospital traumatic cardiac arrest were included. The majority of the patients were adults, female, suffered penetrating trauma (64%) and were in a non-shockable rhythm. Prehospital epinephrine was given to 54% of patients.
Overall, survival to hospital discharge was lower in the epinephrine group (5% vs 16%). In the penetrating trauma subgroup, there was no statistically significant survival difference in patients who received epinephrine and those who did not.
EMS jurisdictions should examine their trauma arrest protocols and consider excluding the use of epinephrine. Several states, such as Maryland, have already removed epinephrine from the trauma arrest protocol.
Following up Dr. Flint's pearl from the other day, the largest study to date looking at a lower Mean Arterial Pressure (MAP) target in elderly ICU patients is the “65” Trial, published in JAMA in 2020. This trial compared a MAP target of 60-65 to the usual goal of >65, in critically ill patients age 65 and older. It included 2,455 patients in 65 ICUs in the UK, and found no difference between the groups.
Bottom Line: Although most intensivists still target a MAP > 65 regardless of patient age, you do have some evidence to support you if you want to target 60-65 in patients over age sixty-five. However, there are some important limitations (well outlined in the PulmCrit article linked below), and therapy should always be optimized to the patient and markers of end organ perfusion.
An open label pragmatic study in 29 Japanese hospitals randomized septic shock patients over age 65 to either a high (MAP 80-85) or control (65-70) group. They then looked at all cause 90 day mortality. The study was stopped early due to a significantly higher percentage of mortality in the higher MAP group.
The study isn’t blinded and is only done in one country, however it does raise the question of what is the ideal MAP for older septic shock patients.
{kind=link}
{kind=link}
{kind=link}
{kind=link}